|
|
Appointments: +91 9137 224 522/ +91 8104 696 654 Emergency: (+91 22) 25763323 Information Helpline: +91 9833 228 602 |
|
|
| Book Appointment | |||
Hip Procedures / Total Hip Replacement |
The hip joint is a ball and socket joint where ball of the thigh bone (femur) joins with the socket (acetabulum) of the pelvic bone. The ball is normally held in the socket by very powerful ligaments that form a complete sleeve around the joint (the joint capsule). The capsule has a delicate lining (the synovium). The ball is covered with a layer of smooth cartilage which is a fairly soft, white substance. The socket is also lined with cartilage. This cartilage cushions the joint, and allows the bones to move on each other with very little friction. |
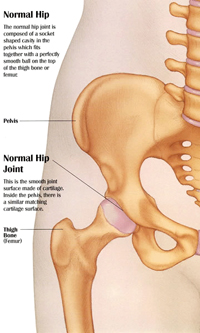 |
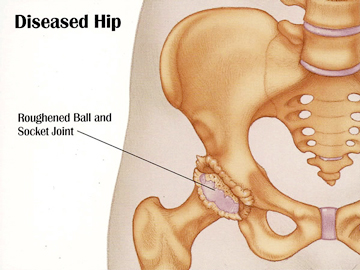
| An x-ray of the hip joint usually shows a "space" between the ball and the socket, which in reality is the gristle (cartilage) because, the cartilage does not show up on x-rays. In the normal hip this "joint space" is approximately 5mm wide and fairly even in outline. This joint space, on the x-ray, reduces significantly when the hip joint is diseased, most commonly due to arthritis (osteoarthritis). Other conditions, such as avascular necrosis and bone tumours also may lead to breakdown of the hip joint and the need for hip replacement surgery. hipkneesurgery |
 |
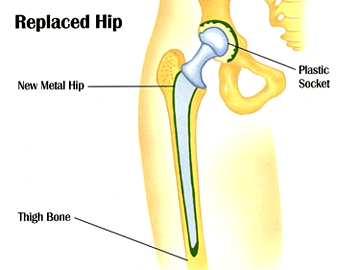
| Total hip replacement is a surgical procedure in which the surgeon replaces the ball (head of the femur) and the socket (acetabulum) with new, artificial parts, called prostheses. Hip replacement surgery usually lasts 1 to 2 hours. The new hip is made of materials that allow a natural, gliding motion of the joint. The goals of hip replacement surgery are to improve mobility by relieving pain and improve function of the hip joint. |
 |
| Usually, people do not spend more than 5-7 days in the hospital after hip replacement surgery. Full recovery from the surgery takes 2 to 3 months, some times more, depending on the type of surgery, the overall health of the patient, and the success of rehabilitation. |
What to expect as a patient of THR |
You are examined by me and, if suitable, a decision to proceed with THR surgery is made. This is a co-operative decision between you, me, your family and your local doctor. The whys and wherefores of this surgery are discussed in detail with you. Main benefits to be expected of this surgery are |
• |
Reduced hip pain |
• |
Enables you to sleep without pain. |
• |
Improved quality of life, ability to return to normal activities. |
• |
Return to sports such as tennis, golf, bowls, cycling, gentle snow skiing and walking. It is not advisable to be running following a total hip replacement. |
| Pre-operation | |
• |
You will be sent for routine blood tests and any other investigations required prior to your surgery a week before surgery. |
• |
You will be asked to undertake a general medical check-up with a physician.
|
• |
You should have any other medical, surgical or dental problems attended to prior to your surgery.
|
• |
Stop smoking as long as possible prior to surgery.
|
| Day of Surgery | |
• |
You will be admitted to hospital usually day before or on the day of your surgery.
|
• |
Further tests may be required on admission.
|
• |
You will meet the nurses and answer some questions for the hospital records.
|
• |
The anaesthetist will discuss with you the type of anaesthetic. Anaesthesia may be either general or regional.
|
• |
Usually the anaesthetist will either sedate you or give you a full anaesthetic if you have a spinal/epidural procedure.
|
• |
You will be given hospital clothes to change into.
|
• |
Approximately 30 minutes prior to surgery, you will be transferred to the operating theatre.
|
Surgery |
Surgery essentially involves exposure of the diseased ball and socket joint and replacing both joint surfaces with man-made, artificial components called prostheses. There are two types of fixation of components to the parent bone, (a) cemented fixation or (b) uncemented fixation. An uncemented fixation allows bone to grow into it. In the recent years, uncemented components have shown very impressive results and, as a result, I prefer to do uncemneted hip replacements, no matter what the age is, unless local conditions dictate otherwise. Following insertion of the components the wound is closed usually with absorbable sutures inside and a drain is inserted. Skin usually gets removable sutures. |
Post Operation |
You will wake up in the recovery room with a number of monitors to record your vital signs such as blood pressure, pulse, oxygen saturation and temperature. You will have a dressing on your hip and a drain coming out of your wound. Post-operative x-rays will be performed in recovery. Once you are stable and awake you will be taken back to the ward. You will have one or two drips in your arm for fluid and pain relief. This will be explained to you by your anaesthetist. On the same day, or occasionally, day following surgery, your drains will be removed and you will be allowed to sit out of bed or walk under the supervision of a physiotherapist. You will be able to put all your weight on your hip, unless conditions dictate otherwise, and your physiotherapist will help you with the post-op hip exercises. You may experience some pain and discomforts, which will be kept under control with medications, but if you are in a lot of pain, inform your nurse. Based on my training and experience from a high volume hip surgery unit in Cambridge, England, I am persuaded to believe that patients may be permitted to mobilise as soon as they can, as the hip allows them to do so. There are really no major restrictions on mobilisation and, it is important to mobilise as soon as you are comfortable as this will prevent complications such as deep vein thrombosis and chest infections. You will be discharged to go home approximately 5-7 days depending on your mobility and help at home. Sutures are usually removed at two weeks |
Risks and complications of hip replacement surgery |
Surgery is not a pleasant prospect for anyone, but for people with arthritis, it could mean a major difference between leading a normal life and putting up with a debilitating condition. Total hip replacement is arguably the most successful procedure in orthopaedic surgery, backed by solid statistics and, evidence shows that the benefits of total hip replacement surgery far outweigh the potential disadvantages. However, as with any major surgery, there are potential risks involved. It is important that you are informed of these risks before the surgery takes place. Anaesthetic complications. As anybody undergoes general or regional anaesthesia, there are risks associated with it although, with technology as it is today, the chances of having a major anaesthetic complication are rare. The risks of course, are magnified if you have abnormal general medical conditions of your vital organs such as heart, lungs and kidneys. Therefore a complete evaluation of those systems has to be performed before you are taken to the operating theatre Blood clots (Deep Vein Thrombosis). These can form in the calf muscles and can travel to the lung (pulmonary embolism). These can occasionally be serious and even life threatening. If you get calf pain or shortness of breath at any stage, you should notify your doctor. Being fully aware of the debate, I take full precautions and I use aspirin 75 mg daily for four weeks, after surgery, as a prophylactic dose. Infection. Superficial wound infections may occur early on and deeper infections can occur at a later stage. The incident of infection is less than 1%. Infections are usually treatable with antibiotic treatment. You are given antibiotics before the operation and for the first two days to prevent infections from happening. Very rarely, if a joint has a deep infection that cannot be controlled with antibiotic therapy, the joint requires removal and a second joint re-implanted at a later stage. Leg length discrepancy. It is not unusual for there to be up to 1cm leg length discrepancy following a total hip replacement. This is quite easily tolerated. Initially you may think that you have a longer leg but this is often due to muscle contracture which over time will loosen up and your leg lengths will even out. Hip dislocation. The risk of hip dislocation is usually less than 1 or 2%. Provided the components are placed correctly and the appropriate post-operative precaution measures adhered to, it is unlikely that the hip will dislocate. Fractures. Very rarely the femoral bone may fracture at the time of surgery and this is usually treated immediately. It is also uncommon to fracture following a total hip replacement unless you have been involved in a bad accident. Loosening of the prostheses. As mentioned, over a period of time the prostheses may loosen if the bone does not grow into it sufficiently or if the bearing surface wears out to produce areas around the prostheses, leading to loosening. Should a prosthesis loosen, then it can be revised. If only the bearing surface wears out, then usually only the bearing surface requires revision which is a much smaller operation. Patients who have metal-on-metal articulating surfaces have a slightly higher metal ion level in their blood. This has been extensively researched over the past 30 years and there have been no increased incidents of cancer or any other problems. Damage to nerves and vessels. It is unusual to damage any major nerves or blood vessels following a hip replacement. However nerve palsy can develop if the nerve is stretched during surgery. Those with hip dislocations from childhood are at higher risk of nerve injury. Haematoma. Occasionally a bleed may occur around the hip joint following the operation that may require drainage. Scarring. Some patients tend to scar more than others and it may be that the scar that you have will be quite thickened (keloid). Long-term swelling. Occasionally the operated leg may remain a little swollen for a number of months but in general this tends to resolve. Numbness around the wound. It is quite possible to get numbness around the wound. It may be temporary or permanent but, this should not affect the function of your hip in any way. Trochanteric bursitis. Occasionally following hip replacement surgery one can experience inflammation at the side of the hip joint which usually settles with either a cortisone injection or anti-inflammatory medications. Joint stiffness. Very rarely extra bone can form around your hip joint which will cause it to stiffen up again (heterotopic ossification). This is usually painless but may cause some stiffness. |
General advice after hip replacement surgery |
You should have a regular check every year with an x-ray. If you have had any major bowel, bladder or dental surgery, antibiotic cover should be given prior to the surgery. Metal prostheses can activate security alarms at the airports. |
Home | Know your Surgeon | Hip Procedures | Knee Procedures | Publications | Lectures | Gallery | Platelet - Rich Plasma Therapy | Contact us